

 Professor Anthony Lawler, Australian Government Chief Medical Officer,
Professor Anthony Lawler, Australian Government Chief Medical Officer, 





 Jess Hadley, community pharmacist and Professional Officer at PDL[/caption]
Jess Hadley, community pharmacist and Professional Officer at PDL[/caption]
 Peter Guthrey, Senior Pharmacist – Strategic Policy at PSA[/caption]
Peter Guthrey, Senior Pharmacist – Strategic Policy at PSA[/caption]


Flu cases surge to record highs as vaccination rates stall
While community pharmacists have smashed previous early-season influenza vaccination records, national coverage still lags dangerously.

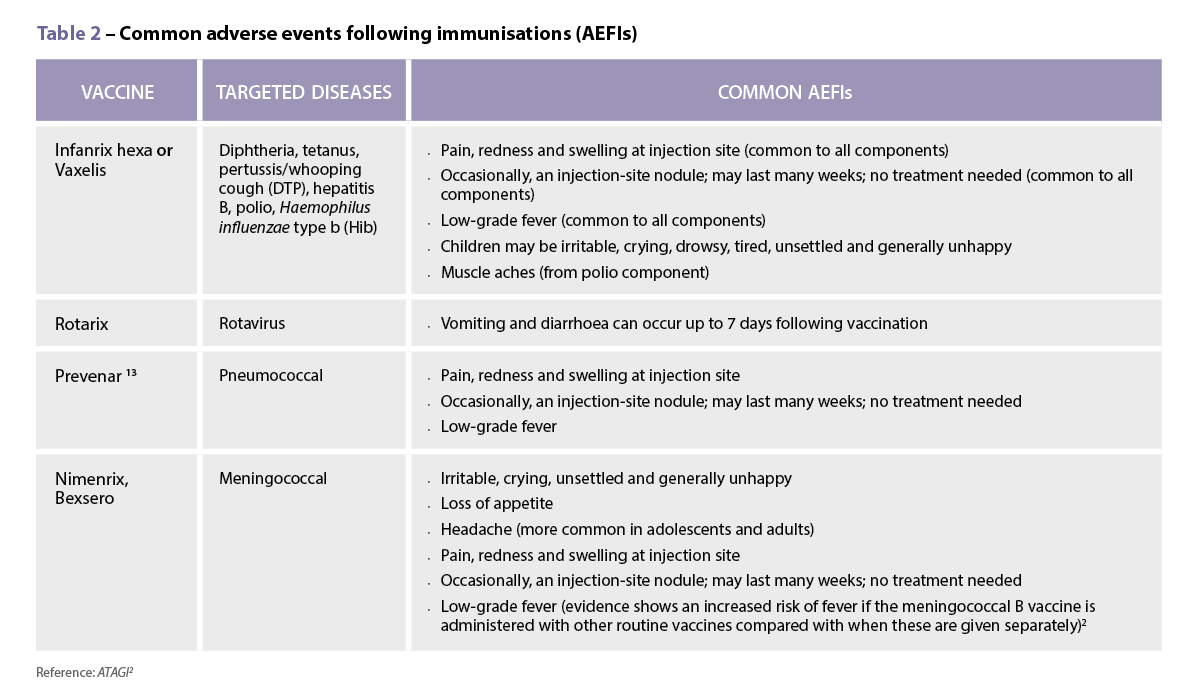
Managing pain and fever associated with childhood vaccination
Routine childhood vaccinations can sometimes be associated with mild adverse effects. Understanding how non-pharmacological strategies and medicines are used to treat pain or fever episodes in this patient cohort is essential.

Mental health missionary
Maria Cooper MPS, PSA’s South Australian Early Career Pharmacist of the Year, is on a mission to improve young pharmacists' mental health.

What happens when patient identification goes wrong?
Identifying patients should be a routine task, but missteps have occurred at an increased rate, sometimes leading to disaster.

Therapeutic Guidelines overhaul UTI treatment
Expansive changes have been made to the Therapeutic Guidelines on antibiotics, encompassing over 1,400 drug recommendations.
Flu cases surge to record highs as vaccination rates stall
While community pharmacists have smashed previous early-season influenza vaccination records, national coverage still lags dangerously.
Managing pain and fever associated with childhood vaccination
Routine childhood vaccinations can sometimes be associated with mild adverse effects. Understanding how non-pharmacological strategies and medicines are used to treat pain or fever episodes in this patient cohort is essential.
Mental health missionary
Maria Cooper MPS, PSA’s South Australian Early Career Pharmacist of the Year, is on a mission to improve young pharmacists' mental health.
What happens when patient identification goes wrong?
Identifying patients should be a routine task, but missteps have occurred at an increased rate, sometimes leading to disaster.
Therapeutic Guidelines overhaul UTI treatment
Expansive changes have been made to the Therapeutic Guidelines on antibiotics, encompassing over 1,400 drug recommendations.
POPULAR
A cup of tea, a Bex and a good lie down

Immortalised in Australian slang, the analgesic phenacetin (used in Bex powder) is wrapped up in the development of the modern pharmaceutical industry and has...
Pfizer COVID-19 vaccine health hubs announced

The Federal Government is calling on community pharmacists to help vaccinate millions of Australians against COVID-19.
Landmark Australian study on oxycodone prescribing

Oxycodone is the most prescribed strong opioid in Australia. Yet little was known about its use and prescribing patterns – until now.
Triptans downscheduled to S3 medicines

Last year, the Therapeutic Goods Administration announced that certain triptans will be available over the counter in 2021.
New CAL D instruction for antibiotics

A new cautionary advisory label for antibiotics that will replace decades of advice to take the medicines ‘until all used’ or ‘until all taken’ will be released next year.
Pharmacists help patients as Ozempic shortage gets even worse

Late last week, the TGA announced there would be no semaglutide stock from mid-November 2022 until the end of March next year.

