

 Professor Anthony Lawler, Australian Government Chief Medical Officer,
Professor Anthony Lawler, Australian Government Chief Medical Officer, 
 Case scenario
Case scenario




 Jess Hadley, community pharmacist and Professional Officer at PDL[/caption]
Jess Hadley, community pharmacist and Professional Officer at PDL[/caption]
 Peter Guthrey, Senior Pharmacist – Strategic Policy at PSA[/caption]
Peter Guthrey, Senior Pharmacist – Strategic Policy at PSA[/caption]


By encouraging open communication and breaking down barriers, pharmacists can help empower women when it comes to their sexual and reproductive health.
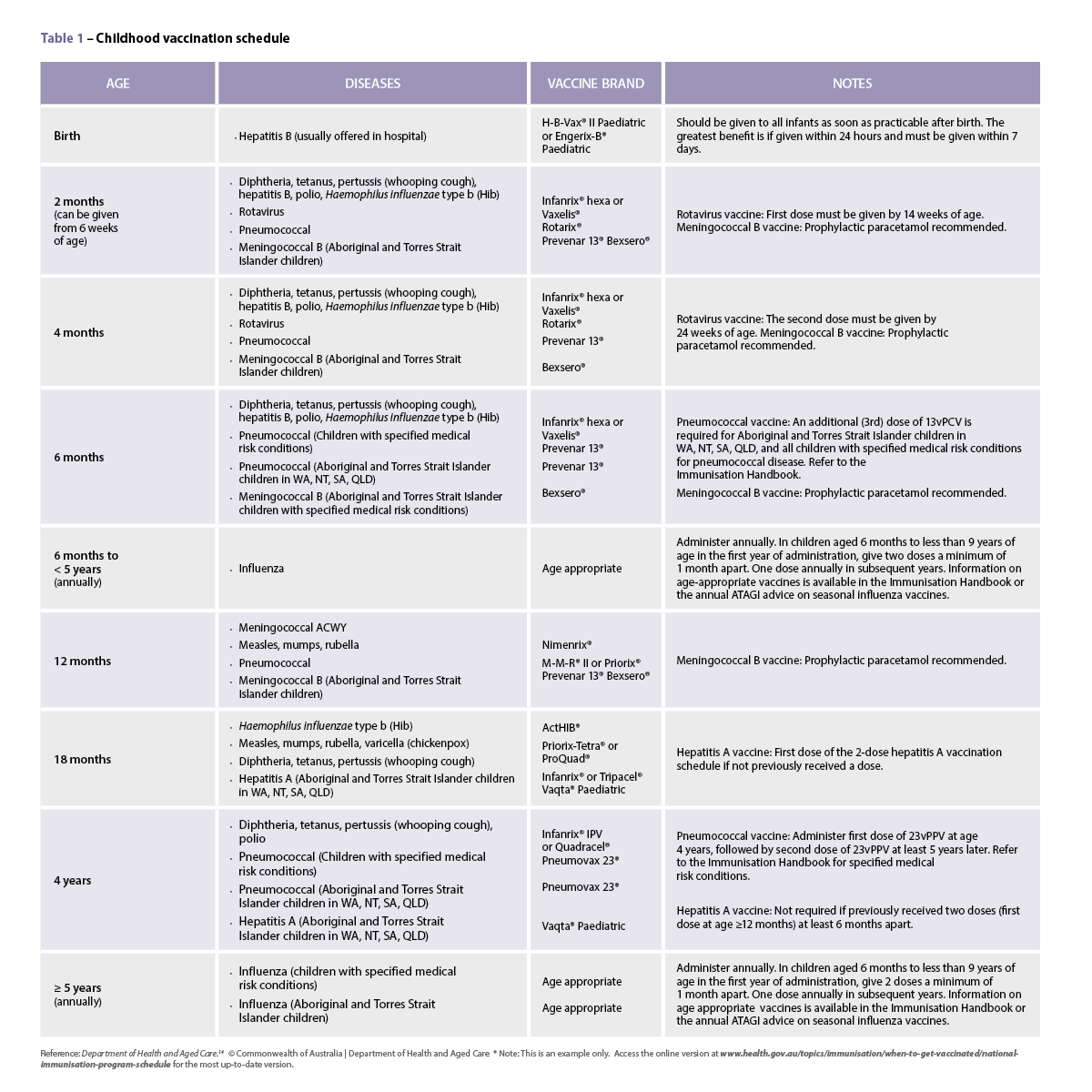
It’s been nearly two decades since pharmacists in 2004 began providing immediate access to the emergency contraceptive pill (ECP) without a prescription as a Pharmacist Only Medicine.
However, unlike in New Zealand and some parts of the United States and United Kingdom, women cannot access the oral contraceptive pill from specially trained pharmacists. Instead they must see a general practitioner (GP) for a prescription.
Those seeking MS-2 Step for medical abortion also face a barrier in the number of GPs certified to prescribe it – 1,345 out of 35,000 practising GPs – as well as finding a pharmacist who is certified to supply and dispense the medicine.
Any pharmacist can register to be a certified MS-2 Step dispenser through MS Health. The certification is pharmacist-specific rather than pharmacy-specific, so every pharmacist who dispenses MS-2 Step in a particular pharmacy must be certified.
‘Women in Australia currently experience structural (for example, financial and geographical), personal (lack of knowledge) and provider-related (biases or conscientious objection) barriers to accessing comprehensive contraception services,’ says Pip Buckingham, PhD candidate and researcher for the Centre of Research Excellence in Sexual and Reproductive Health for Women in PrimaryCare (SPHERE).
This situation has worsened during the pandemic, says Ms Buckingham, whose research focuses on broadening women’s contraceptive choice in general practice and pharmacy.
Indeed, a 2020 report by Marie Stopes Australia into sexual and reproductive health rights in Australia found access to contraception and emergency contraception, and pregnancy and sexually transmitted infection (STI) testing, was reduced due to COVID-19. This inequity has been greater for people who already experience barriers to healthcare, including Aboriginal and Torres Strait Islander people, migrant and refugee communities, young people and those living in regional, rural and remote areas.
Rates of unintended pregnancy are also disproportionately higher among women who are socio-demographically disadvantaged and those living outside metropolitan regions.
Pharmacists can address many of these barriers and present a number of opportunities for accessible contraceptive counselling, products, screening for STIs and medical abortion.
TAREN GILL FPSPriceline Pharmacy, Maryborough, Vic We’re in a country town where everyone knows everyone. There are only two pharmacies in Maryborough and only ours is open on a Sunday. We’ve had teenagers come in to get emergency contraception and they don’t want everyone to know – that is one of the barriers we have to overcome. One of the ways we try to be more discreet is to have a card (above) in the feminine hygiene section of the pharmacy that says ‘Secret Women’s Business’. It explains that if you want to talk to the pharmacist, you just need to deposit the card at the counter. We have contraceptive conversations with teenagers who don’t want their parents to know, and I give a talk to Year 10 girls at the local high school about sexual and reproductive health. I like to think that grassroots education helps to increase awareness around these issues and helps empower girls to take control That said, we make sure women who come into the pharmacy looking for contraceptive advice are aware that contraception comes in many forms, including IUDs and implants, and that this is something they can discuss with their doctor. For example, as the contraceptive pill requires a lot of compliance, a 3-month injection may be a better option. When women come in to access emergency contraception, we try to find out more about their cycle, or what’s going on for them. One of the most common groups looking for this type of help is happily married women with multiple kids who don’t want any more. There is no need for stigma and judgement about the reasons a woman wants to access emergency contraception. We don’t have a prescriber in town for MS-2 Step. The nearest pharmacy is Ballarat or Bendigo [about 70 kilometres away]. I would feel comfortable about having some forms of contraceptive pill available over the counter if I was able to assess that the person didn’t have risk factors for side effects such as a clot, or wasn’t a smoker or overweight, as they may require closer monitoring. There would be a few things you would need to tick off, and our responsibility as pharmacists is to make sure that the medicines we dispense are safe and efficacious. |
Accessibility issues
It is important that pharmacists feel ready and confident to have discussions about women’s sexual and reproductive health and recognise the actual or perceived barriers women may face, says Stefanie Johnston MPS, PSA’s General Manager – Knowledge Development.
‘PSA has a number of practice support tools, including a Pharmacist Only Medicine guidance document and online education modules to enable pharmacists to upskill in this area,’ she says. ‘Pharmacists are in a great position to provide information to women who have questions about their contraception and what may be the best option for them.’
One barrier is feeling a sense of shame or vulnerability when talking to a pharmacist about emergency contraception, or contraception more generally. A simple solution is to offer patients more privacy, says Ms Johnston. For example, if a woman appears on edge or is constantly looking towards the pharmacy entrance, suggest moving into a consultation
room where others can’t see or overhear the conversation.
A lack of knowledge can also make women feel unsure when it comes to their sexual health, so it is important to explain why you need to ask certain questions when providing certain medicines, Ms Johnson says.
‘It’s rare that emergency contraception isn’t appropriate.’ But there are instances, she adds, where it cannot be taken. This could be due to other health conditions, other medicines or the length of time since unprotected sexual intercourse.
As there may be reduced efficacy of ECPs with increasing body weight, pharmacists should also be prepared to ask potentially confronting questions.
‘If it’s a situation where you feel uncomfortable, rehearsing the conversation and considering how you phrase things could be a good idea,’ Ms Johnston says. ‘For example, “I need to ask you a couple of questions to make sure I give you the right medicine and ensure it is as effective as it can be”. ‘
Counselling patients on emergency contraception also provides an opportunity to increase someone’s knowledge about contraception and sexual health more broadly – but
only if the patient is open to it.
‘You need to meet people where they are. Some people find it a very personal conversation and are embarrassed, while some are happy to talk about it.’
| A PATIENT'S BARRIER | A PRACTICAL RESPONSE |
|---|---|
| Patient is anxious about being seen by someone they know | * Ask if the patient would like to have the conversation in a private consultation room * Offer to talk to the patient on the phone and have the medicine packaged up and ready for collection when she arrives * Place ‘secret women’s business’ cards in the women’s health section of your pharmacy, to encourage patients to start ‘difficult’ conversations * Have signage in the pharmacy and on social media/website that private consultation areas are available |
| Questioning is confronting | * Explain you are going to provide the medicine but must get some information first * For example, ‘I need to ask you a couple of questions to make sure I give you the right medicine and ensure it is as effective as it can be’ * Note: using a paper checklist when dispensing emergency contraception is no longer a routine recommendation, as it represents a barrier to access for some women |
| Request for emergency contraception too long after sexual intercourse | * If too much time has elapsed after sexual intercourse, explain the medicine is only effective within a specific timeframe and the patient will need to see a doctor * Offer to schedule an appointment with a GP |
| You have a conscientious objection to providing the medicine, or the medicine is out-of-stock in your pharmacy | * Pharmacists have an obligation to facilitate access, such as referring the patient to another pharmacist or facility where they can access the medicine |
| Your patient is not a native English speaker | * Use the Translating and Interpreting Service (TIS) to ensure clear communication. Call 1300 575 847 |
EVA QUEK MPSSanctuary Lakes, Victoria We’ve never refused to issue emergency contraception because there isn’t much of a contraindication. Sometimes though, we have had to explain that, because the patient has left seeking advice more than 5 days [after sexual intercourse], it is too late, and they will need to go and see their doctor for a discussion about their options. If this is needed, we might offer to schedule an appointment for them. If is someone whose first language is not English, we have staff members who speak Vietnamese, Greek, Serbian, Hindi and Mandarin. There is also the Translating and Interpreting Service. We also find out about any medicines they are on, and we always counsel them on the adverse effects. We might let them know that a more long-term form of contraceptive, like the oral contraceptive, or an implant, may be a useful consideration and suggest they discuss this with their doctor. As pharmacists, we can provide more information to women who have questions about their contraception. For example, I have spoken to women in the past who have raised concerns about the risks of deep vein thrombosis with certain oral contraceptive pills and they have decided to consider alternative contraception methods, such as a contraceptive implant instead. We have two pharmacists in our pharmacy who are registered to provide MS-2 Step. |



