

 Pharmacists have always prescribed, but they have the potential to prescribe much more
Pharmacists have always prescribed, but they have the potential to prescribe much more



 Sponsorship information
Sponsorship information


 Talking to patients who have questions
Talking to patients who have questions
Most Australians don’t use their asthma inhalers correctly. By distinguishing between the two different types of inspiratory flow rates, this new inhaler label could help to improve a dismal status quo.
Asthma and chronic obstructive pulmonary disease (COPD) are common respiratory conditions with a significant burden of disease.
Around 2.7 million Australians report having asthma, while COPD affects an estimated one in 13 adults over 40 years of age (7.7%) – rising to 29% among people aged 75 years and older.
The mainstay of pharmacological treatment for asthma and COPD is inhaled therapy with bronchodilators and corticosteroids, delivered via:
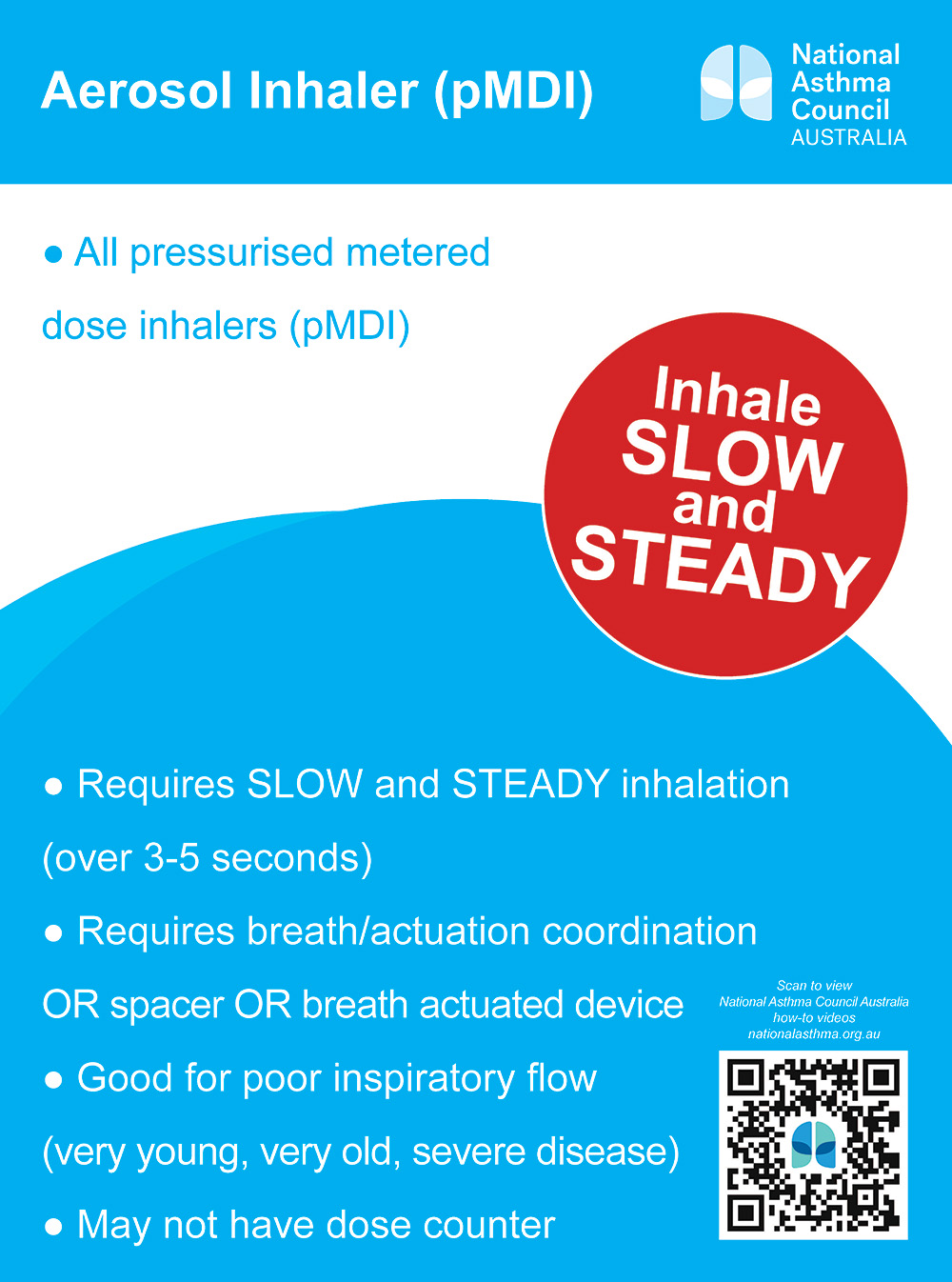
- pressurised metered dose inhalers (pMDIs)
- breath-actuated (BA)-pMDIs
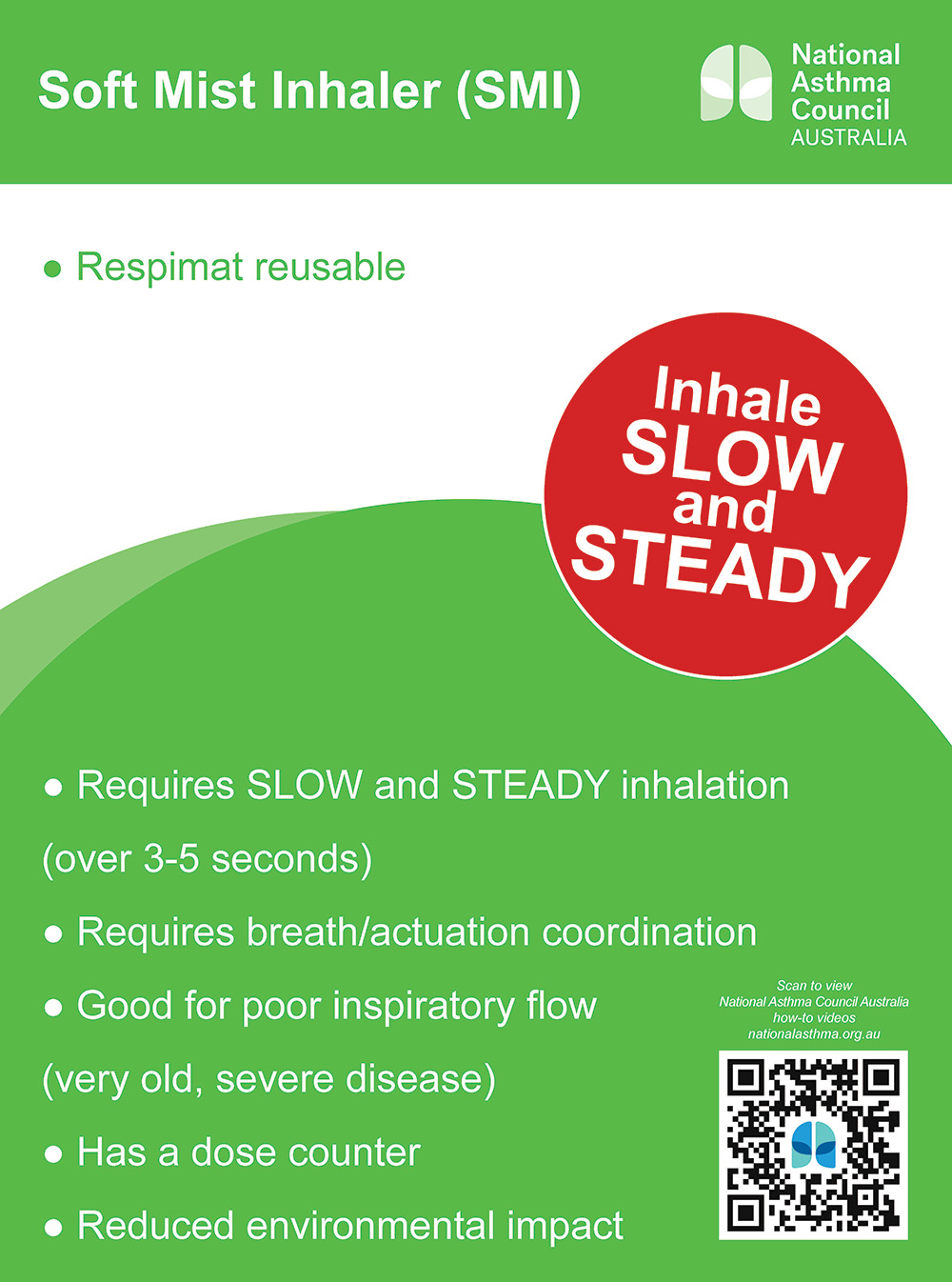
- soft mist inhalers (SMIs)
- dry powder inhalers (DPIs).
Choosing the right device for the individual patient is crucial to ensuring correct technique and improving the likelihood of good adherence – with optimal inhaler technique critical to optimal disease outcomes.
Older age, cognitive impairment, multiple devices and lack of previous training are all risk factors for poor inhaler use and adherence. Not using an inhaler device correctly can lead to:
- inadequate dosing
- suboptimal disease control
- worsening of quality of life
- increased hospital admissions and mortality.
The shocking statistic that 94% of Australians don’t use their asthma inhalers correctly means there is a need for change.

To promote better inhaler technique, the National Asthma Council Australia (NAC) and PSA have developed supplementary labels to be affixed to inhalers in addition to the dispensing label.
Understanding inspiratory flow rate
Inspiratory flow rate – which directly impacts both the amount of drug that is inhaled as well as the lung deposition – is one of the most critical errors patients can make.
But with numerous inhalers available in Australia – each with its own unique optimal peak inspiratory flow rate (PIFR) – it can be extremely confusing for patients, particularly for those on multiple different inhalers.
For pMDIs, BA-pMDIs and SMIs, inspiratory flow rate should be about 30 L/min to minimise deposition in the oropharyngeal area and enhance delivery to the lungs.
However, most people inhale far too quickly using pMDIs when the inspiratory flow rate should be slow, steady and deep over 3–5 seconds for adults and 2-3 seconds for children to minimise deposition in the upper airways and enhance delivery to the lungs.
For DPIs, 60 L/min is generally accepted to be optimal. Children and older adults may have trouble reaching this inspiratory flow rate; however, most patients with COPD are able to generate inspiratory flows necessary for effective DPI use.
Although the optimal flow rate differs between each DPI device due to differences in inhaler design and internal resistance, the principle remains the same for all – a quick and deep inhalation over 2–3 seconds is required to deagglomerate the active ingredient powder from carrier powder (usually lactose) and aerosolise the particles. It’s important that the inspiratory flow rate at the start of the inhalation is forceful, rather than gradually increasing.
The internal resistance of DPIs vary, requiring different inspiratory effort to produce sufficient flow rate. With low resistance devices, patients must inhale faster to generate the power to separate the active ingredient molecules, which may be difficult in patients with poor lung function. Low-resistance DPIs (e.g. Breezhaler) require a minimal inspiratory flow rate of > 90 L/min, whereas medium-resistance DPIs (e.g. Turbuhaler, Genuair, Spiromax, Easyhaler) require 50-60 L/min, and < 50 L/min for a high-resistance DPI.
High resistance devices (e.g. Handihaler) do not require a patient to inhale as fast, so most patients can effectively use these DPIs regardless of age and disease severity.
Where possible, inhaler device polypharmacy should be minimised by use of single-inhaler dual and triple therapy.
Navigating patient conversations
The new labels provide a refreshed opportunity to initiate a different conversation with patients about inhaler technique.

Pharmacists can point out: ‘There’s a new sticker that focuses on how you breathe in and your inspiratory flow rate. Because if you don’t have the correct inhalation technique, you’re not getting the most out of your medicines, and therefore not controlling your asthma or COPD as best as you can.’
When patients are using multiple inhalers with different inspiratory flow rates, for example a DPI and pMDI, a supplementary label can be applied to each, acting as a prompt and reminder about which way they should be breathing in.
Pharmacists could then follow up by saying, say, ‘Did you know the best way to use DPI inhalers is quick and deep inhalation?’ – either demonstrating the process on placebo devices, or showing patients the NAC’s videos on inhaler technique.
When patients understand the importance of something, behavioural change is more likely.
When dispensing DPIs, for example, pharmacists could explain that they don’t contain a propellant like some other inhalers, meaning a quick and deep inhalation is needed to separate the drug from the lactose powder – helping to ensure the active ingredient gets down into the small airways of the lungs.
Pharmacists can then ask patients if they would feel comfortable to demonstrate their inhaler technique on the dispensed devices.
An In-Check Dial – a hand-held device with an adjustable dial to mimic the internal resistance of different inhalers – can be used to identify suboptimal PIFR and help with inhaler device selection and technique training.
Taking every opportunity
While it can be challenging, pharmacists should check patients’ inhaler technique at every opportunity – including the first and at every repeat dispense.
A MedsCheck could be a good way to do this, allowing pharmacists to spend 10–15 minutes with a patient.
At the very least, pharmacists should check patients’ inhaler technique every 6 months and document the discussion in dispensing records.
Resources
Along with the new stickers, asthma inhaler information cards are available to help with appropriate selection of labels, with a QR code linking to the NAC videos on inhaler technique.
APF26 (and APF digital) also has a new and updated section on inhalers ‘Instructions for administration of different dosage forms’, detailing the steps for different types of inhalers.
Pharmacists can visit the NAC exhibition stand at PSA24 to collect the stickers and cards, which are also available here:
Don’t miss Debbie Rigby leading Masterclass 2 – Making the most of living with COPD at PSA24 on Friday, August 2, 2024.


