


 Categorisation of heart failure
Categorisation of heart failure A focus on SGLT2is
A focus on SGLT2is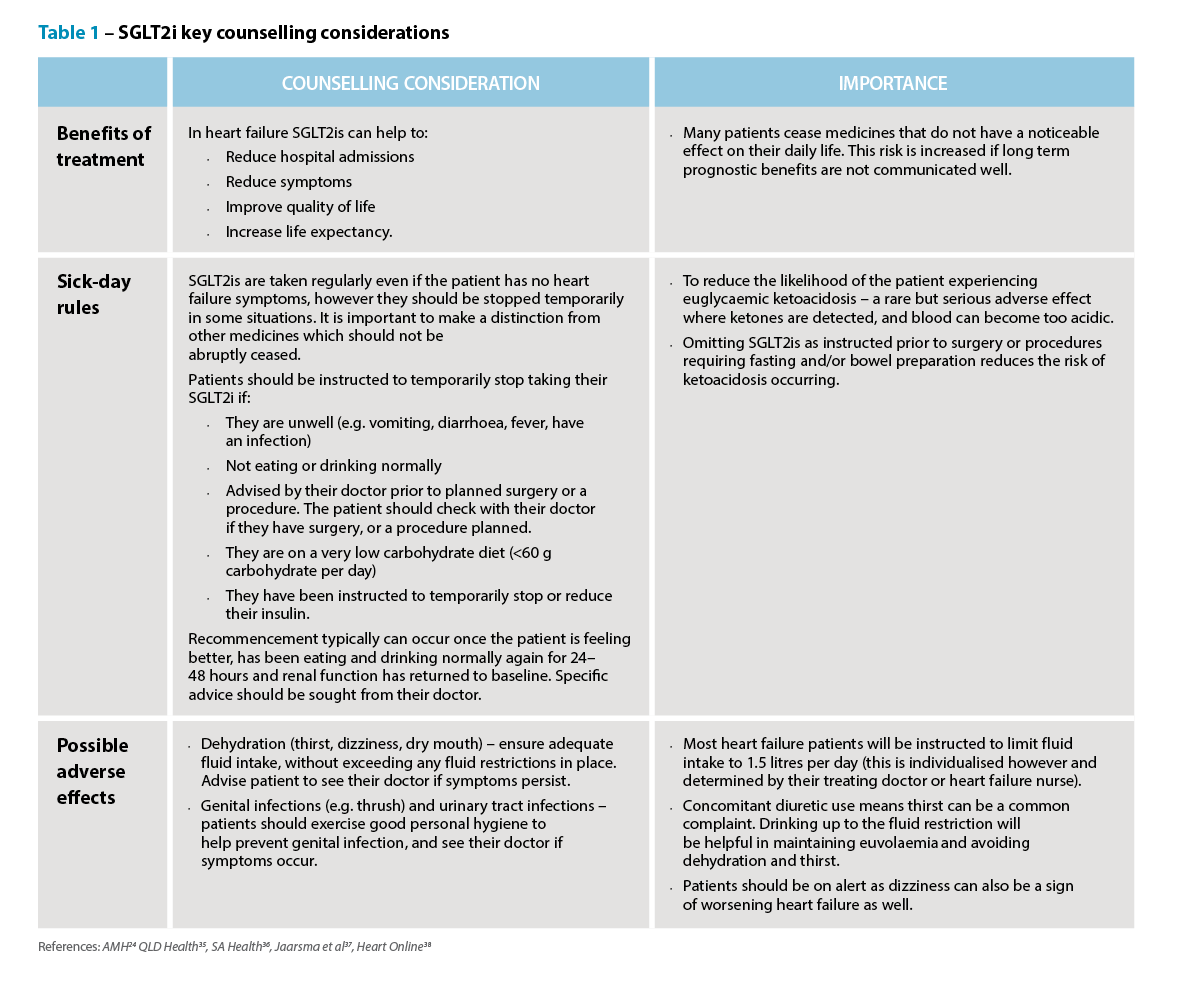 Knowledge to practice
Knowledge to practice 
 Professor Anthony Lawler, Australian Government Chief Medical Officer,
Professor Anthony Lawler, Australian Government Chief Medical Officer, 
 Case scenario
Case scenario




The Fair Work Commission’s Expert Panel for pay equity in the care and community sector has today issued its initial decision on the Gender-based undervaluation – priority awards review – making determinations on the Pharmacy Industry Award 2020, which most...

While community pharmacists have smashed previous early-season influenza vaccination records, national coverage still lags dangerously.

Identifying patients should be a routine task, but missteps have occurred at an increased rate, sometimes leading to disaster.

There have been two deaths in the southwest US due to measles. Western Australia is facing a fresh outbreak. Are we next?

PSA's inaugural GP Pharmacists Symposium underscored the expanding scope of the profession – and the policy gaps that still need closing.

This state just made pharmacist prescribing permanent, with others to follow. Here's what pharmacists need to know to embrace this new role.

From prescribing rights to aged care roles, the 2025 federal election could usher in pharmacy-led healthcare reform.

New major review finds that antidepressants used for back pain and sciatica can cause more harm than good.

Several women’s health medicines will be on the Pharmaceutical Benefits Scheme after new PBAC recommendations.

The Therapeutic Goods Administration issued an alert over a commonly used of broad-spectrum class of antibiotics.

