

 Professor Margie Danchin[/caption]
Professor Margie Danchin[/caption]

 Dr Peter Tenni[/caption]
Dr Peter Tenni[/caption]
 How should we deprescribe gabapentinoids, according to the Maudsley Deprescribing Guidelines[/caption]
How should we deprescribe gabapentinoids, according to the Maudsley Deprescribing Guidelines[/caption]



 Pharmacists have always prescribed, but they have the potential to prescribe much more
Pharmacists have always prescribed, but they have the potential to prescribe much more
Turning informal advice into a structured consultation service: pharmacy-based travel health services take flight.
Australians love to travel and they take off to all parts of the globe, whether it be safaris in Africa, a bargain trip to Bali, visiting family in India or cruising through the icebergs within the Arctic Circle.
But as the average age of travellers, population density, pollution and zoonotic diseases increase, so, too, do health risks associated with travel.
Pharmacists have long provided ad hoc advice for travellers in response to patient queries, whether it be guidance on how to store medicines during transit or encouraging patients to see a GP, or dedicated travel doctor service in major cities, for vaccination.1
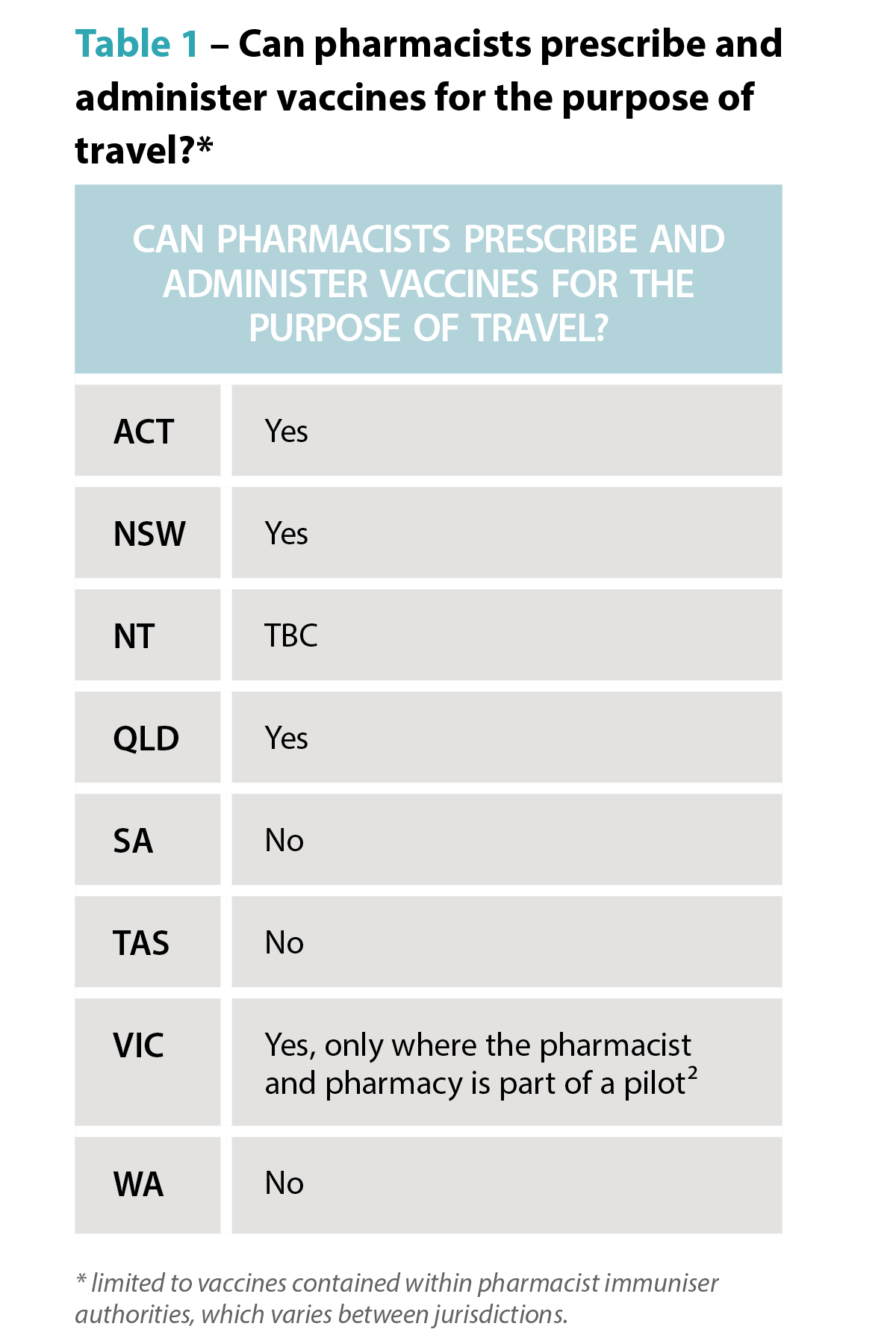
But with more Australians jetting off to more locations more frequently, more travel health services are needed. Some pioneering pharmacists are leading the way. Enabled by an increasing range of vaccines pharmacists can both prescribe and administer as well as formal pilots and programs from state governments, community-pharmacy based travel health consultation services are taking flight.
How does a formal travel health service differ from ad hoc advice?
Put simply, its more comprehensive. It considers a much wider range of risks than the patient may self-identify and makes recommendations to the traveller proportional to their individual needs.
‘Outside of a formalised program like the Victorian Community Pharmacy Statewide Pilot project,2 the pharmacist may not go into as much depth about [travel health] matters because there’s an expectation the consumer’s GP will have that discussion when a patient asks about vaccines,’ says PSA Victorian State Manager Jarrod McMaugh MPS.
It means pharmacists ‘instead of picking and choosing pieces of information they’re going to add on to a consultation before referring and saying “go to see your GP for these things”, they’re going to address them all directly in a travel health service’, he says.
And to be comprehensive the service needs a deep understanding of the traveller(s), when/where they are going, how they are going to get there – e.g. cruise, fly, drive, trek – and the types of things they’ll do when they are there.

Getting started
Establishment or formalisation of any service has common features: staff training, developing standard operating procedures, setting up documentation systems and advertising. However, a travel health service has two additional aspects, which are critical to success.
Firstly, the practitioners need to really wrap their heads around international travel, the health risks a person is likely to encounter and how to craft a valuable consultation for each traveller.
‘Some pharmacists are avid international travellers, and will have generated substantial knowledge of destinations, transport routes and product availability at pharmacies overseas. This expertise is advantageous in providing bespoke, individualised advice,’ Mr McMaugh says.
‘For example, Australians are often surprised by the high cost of sunscreens overseas, or how unpleasant the taste of oral rehydration products available in other markets are.’
‘Additionally, people often overlook prohibitions on carrying common medicines through common transit points such as Middle Eastern or Asian airport hubs.’
These kinds of insights may not be front-of-mind for travellers when booking in for a consultation, but they are important for risk mitigation and highly valued.
Also important is anticipating risks for which travellers may not be alert. For example, a family holiday to a Thailand beach resort may initially seem lower risk, but activities and excursions where you interact with wildlife such as monkeys are common and carry zoonotic infection risk.
 For pharmacists who do not have this knowledge from primary experience, seeking these reflections from colleagues or through careful listening with patients is essential.
For pharmacists who do not have this knowledge from primary experience, seeking these reflections from colleagues or through careful listening with patients is essential.
Structuring a consultation is something each practitioner needs to find their own way to master. Unlike other services, the approach to these longer consultations isn’t so black and white.
Compared to other expanded scope programs, travel health requires mastering the navigation of the grey.
One of the hundreds of pharmacists offering a travel service under the Victorian pilot is Melbourne’s Tooronga Amcal Pharmacy owner Andrew Robinson MPS, who reflected that ‘[with a UTI treatment service], we follow a protocol guideline and it’s more straightforward to undertake’. With travel, it is like a Pandora’s box that you can open and find you going all over the place with a whole lot of different destinations, a whole lot of different complications, a lot of different needs.’
Finding prospective travellers
A common theme with all pharmacists contacted by AP is that the identification of patients who would benefit from the service has initially been more successful through conversations in patient interactions than via formal advertising.
The trigger for knowing a patient could benefit from a sit-down travel health consultation with a pharmacist could be anything, Mr McMaugh notes.
‘It can literally be a comment in passing: ‘My son is about to travel overseas for the first time.’
Other queries could be related to how to carry medicines safely overseas, or interest in medicines for motion sickness.
Andrew Robinson describes the trial as a ‘significant endorsement by health regulators that pharmacists are capable of delivering more complex services.
‘Before actually doing an appointment, you’ve got to tease it out a bit first. It’s not like some of the other pilot programs that we’ve done, which are very, “you’ve got a urinary tract infection. You fit the criteria. We can undertake the consultation”.’
‘In contrast, you almost need to do a [travel health] consultation to find out whether you need to refer them on. So, I try and garner that before. But I think if we boil it down and keep it simple, the reality is there’s plenty of people out there who are not thinking about travel health that need a typhoid vaccine and a bit of a conversation,’ he said.
 Mr Robinson identified that consumers who, at short notice, book a trip to south-east Asia and don’t plan a GP visit have particularly welcomed his travel health consultations.
Mr Robinson identified that consumers who, at short notice, book a trip to south-east Asia and don’t plan a GP visit have particularly welcomed his travel health consultations.
‘We see this particular pilot really looking at the high-risk patient, the person who sees a cheap flight to Indonesia and in 3 weeks’ time they’re gone. They think of it as just a great way to relax and give very little thought to the risks associated with that travel.’
Susannah Clavin MPS, the owner of the Marc Clavin Pharmacy at Sorrento on Victoria’s Mornington Peninsula, regularly discusses travel health with patients and consumers, and has had success with online bookings.
‘Most [patients] were heading to south-east-Asia. They are all very time-poor, so if the pharmacy is closely located to their home or workplace then I think they will appreciate the convenience. Being able to book online, too, is a bonus.’
Like Mr Robinson, Ms Clavin had also identified patients through conversations at the dispensary.
‘One of the patients had a prescription for the vaccine and asked us for a quote,’ recalls Ms Clavin. ‘We gave the quote and mentioned that we could also administer the vaccine, for a fee. [The patient] was very keen to save a trip to the doctor.’
Fee-for-service
How much should the service charge? While each business needs to make its own decision based on the costs of delivery and business policies, experience in travel doctor clinics and within pilot sites shows consumers are willing to pay for the consultation service, which may include administration of vaccines.
When AP spoke to Mr Robinson, he had conducted about a dozen travel health consultations, charging $50 for a half-hour consultation. Families travelling overseas, he says, have found the consultations particularly attractive because the pharmacist can give advice to an entire family in one appointment.
Looking to the future
Feedback from the Victorian trial shows an effective travel health consultation service is a good fit with pharmacies that have a well-integrated vaccination service, according to Mr McMaugh.
‘If you’re doing the occasional vaccine, you have to change gears, going from doing whatever other services or dispensing you were doing, to administering the vaccine and then coming back into the retail and dispensing space,’ he says.
Mr Robinson hopes travel health consultations become a permanent fixture in the service landscape for pharmacy.
‘Travel is all about having fun. But we need to make sure it stays fun, and you stay healthy, because otherwise it’s a very expensive holiday.’
 The rise of zoonotic diseases
The rise of zoonotic diseases
Where a person is travelling to and where they are staying matters. A trip to Zimbabwe to see Victoria Falls has a very different risk profile to a walking safari at remote campsites. Similarly, holiday resorts in south-east Asia next to agricultural fields have a different risk profile to city hotels.
Recent decades have seen the rise and reemergence of viral zoonotic diseases.4 The growth of tourism has led to land changes, travel patterns and farming practices which increase the risk of zoonotic diseases, including novel and well-established pathogens.⁵
Travellers and health professionals alike need to keep abreast of these trends. Rabies is a good case in point. The USA continues to log around 4,000 animal rabies cases each year, with >90% of cases from bats, raccoons, skunks and foxes – a shift from the 1960s where dogs were the primary rabies risk to humans.⁶ In contrast, dog bites are the predominant source of rabies infections in Africa.⁷
Karen Carter FPS, partner of Carter’s Pharmacy Gunnedah and owner of Narrabri Pharmacy in north-west NSW, can now offer rabies vaccinations.
‘You think of exotic animals for rabies but sometimes it’s dogs that people are at risk of being bitten by,’ Ms Carter says.
The vaccine isn’t cheap, so considering the exposure risk and access to post-exposure prophylaxis is important when discussing the benefits of the vaccine with patients.
‘We had a gentleman travelling to Africa and then on to South America for his work in the agriculture industry, so we recommended he get the rabies vaccine.’ Ms Carter says. In fact, he not only got the rabies vaccine administered, but the hepatitis A and typhoid vaccines as well before he left.
‘We were also able to refer him to a Tamworth GP clinic for his yellow fever vaccines, Ms Carter adds. ‘He thought it was great that we could do all but one of his vaccines in the pharmacy.’
Other zoonotic infections, such as mpox, avian influenza and Japanese encephalitis also have changing patterns of transmission and distribution, which increasingly require consideration in travel health services.
Case study
 Dat Le MPS Owner, Priceline Pharmacy, Knox, Melbourne VIC
Dat Le MPS Owner, Priceline Pharmacy, Knox, Melbourne VIC
This traveller
Mrs L, a 62-year-old regular dose administration aid (DAA) patient, is living with gastro-oesophogeal reflux disease (GORD), hypertension, atrial fibrillation, high cholesterol and osteoarthritis in the knee.
Current medicines
- pantoprazole 20 mg once daily
- moxonidine 200 microgram once daily
- apixaban 5 mg twice daily
- simvastatin 20 mg at night
- paracetamol 1330 mg three
times a day
Vaccination history
- COVID-19: >12 months ago
- Influenza: Up to date
- No other AIR history.
This trip
She’ll be leaving in a month and will be away for 7.5 weeks staying in metropolitan area hotels in both Vietnam and Thailand. Mrs L is travelling on direct flights from Melbourne with no transit points.
This time
Mrs L explains that it will be summer when she arrives in both south-east Asian countries.
Recommendations
Based on her travel plans, I recommend vaccination for:
- COVID-19 (administered into her
right arm) - hepatitis A (administered into her left arm)
- typhoid (administered into her left arm).
Mrs L was advised she would have full protection from hepatitis A in 2 weeks and that it may be at least a week before the COVID-19 booster provided full protection.
She was also told that the vaccinations may cause sore arms, some redness, fever or chills.
While her typhoid vaccination would protect her for 3 years, she could have another COVID-19 booster in a year.
For the hepatitis A vaccine, a typical course is two doses – the first at day 0, and the second from 6 months later, ideally before 12 months, if she travels again within the year.
Rehydration preparations were also recommended, along with hand sanitiser, face masks and sunscreen for Mrs L’s holiday group tour to various sight-seeing locations.
When she collected her DAAs, we advised Mrs L how to store her medicines. She was pleased she didn’t need to make a GP appointment, organise vaccine prescriptions, collect them at the pharmacy and then take them back to the doctor to be administered. I reminded her that we would call her about her second hepatitis A dose to complete her course.
We put a note on her next DAA collection asking about her holiday and any problems she may have had such as diarrhoea or tablet storage problems.
References
- Pharmaceutical Society of Australia. Travel health: essential CPE. Deakin, Canberra: 2023. At: https://my.psa.org.au/s/training-plan/a110o00000KVhisAAD/travel-health-essential-cpe
- Department of Health, Victoria. Travel Health and vaccination. Community pharmacist statewide pilot – patient handout. 2024. At: health.vic.gov.au/primary-care/victorian-community-pharmacist-statewide-pilot-resources-for-pharmacists
- Queensland Government Queensland Health. Queensland community pharmacy pilots. 2024. At: health.qld.gov.au/clinical-practice/guidelines-procedures/community-pharmacy-pilots/about#scope
- Marie V, Gordon ML. The (Re-)Emergence and spread of viral zoonotic disease: a perfect storm of human ingenuity and stupidity. Viruses 2023;15(8):1638.
- Esposito MM, Turku S, Lehrfield L, et al. The impact of human activities on zoonotic infection transmissions. Animals (Basel) 2023;13(10):1646.
- Centres for Disease Control. Rabies. 2024. At: www.cdc.gov/rabies/php/protecting-public-health/index.html
- MbiloC, Coetzer A, Bonfoh B, et al. Dog rabies control in west and central Africa: a review. Acta Tropica 2021;224:105459.


